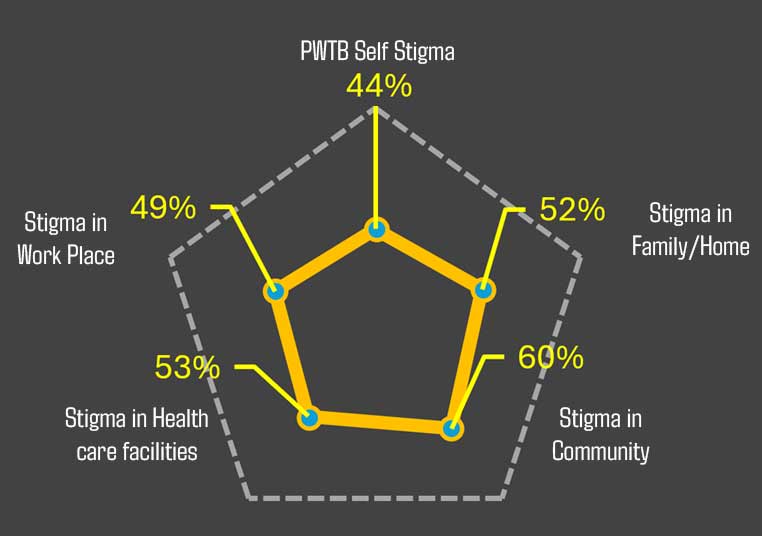







 Real-Time Data on TB
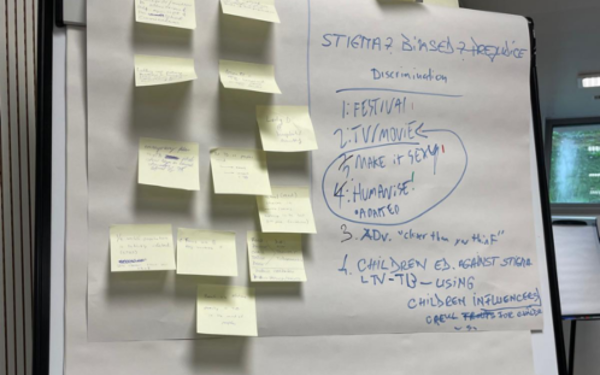
Stigma
Real-Time Data on TB
Stigma

Lorem ipsum dolor sit amet, quo ei simul congue exerci,


My Page

In this example, the sidebar is hidden (style="display:none")
It is shown when you click on the menu icon in the top left corner.
When it is opened, it shifts the page content to the right.
We use JavaScript to add a 25% left margin to the div element with id="main" when this happens. The value "25%" matches the width of the sidebar.